ApoB vs. LDL: The Cardiovascular Marker Most Clinics Aren't Ordering
ApoB predicts cardiovascular risk more accurately than LDL cholesterol — but most clinics don't order it. Dr. Victor Calvo of Provena Care Miami explains what ApoB measures, why it matters, and what your result means.
APOBLDLCARDIOVASCULAR HEALTHCHOLESTEROLHEART HEALTHLONGEVITYMIAMI
Dr. Victor Calvo, MD
5/18/20266 min read
ApoB vs. LDL: The Cardiovascular Marker Most Clinics Aren't Ordering
By Dr. Victor Calvo, MD — Medical Director, Provena Care Longevity · Cardiovascular Health · Miami, FL
Why Your Cholesterol Panel May Be Missing the Most Important Number
For the past five decades, LDL cholesterol has been the primary target of cardiovascular risk management. Statins are prescribed to lower it. Dietary guidelines are built around it. Patients are told their heart risk is low or high based largely on this single number.
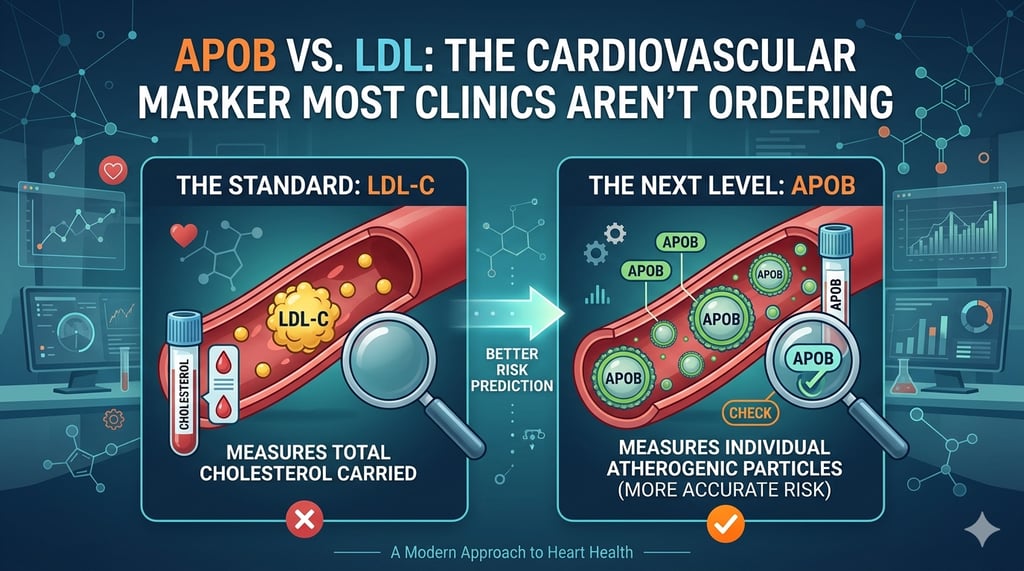
The problem is that LDL cholesterol — as measured on a standard lipid panel — is a concentration measurement, not a particle count. And it is the number of particles, not the concentration of cholesterol within them, that most accurately predicts who will develop atherosclerosis.
ApoB — apolipoprotein B — is the protein that coats every atherogenic lipoprotein particle in the blood. One ApoB molecule per particle means that measuring ApoB gives you a direct count of every LDL, VLDL, IDL, and Lp(a) particle in your circulation. It is, by multiple lines of evidence, a more accurate predictor of cardiovascular risk than LDL cholesterol.
It is also absent from the standard lipid panel ordered at most primary care visits.
This article explains what ApoB is, why it matters more than LDL in many patients, how to interpret your result, and why Provena Care includes it in advanced metabolic assessments.
The Problem With LDL Cholesterol as a Risk Marker
Standard LDL measurement is not directly measured in most clinical labs. It is calculated using the Friedewald equation:
LDL = Total Cholesterol − HDL − (Triglycerides ÷ 5)
This calculation becomes inaccurate when triglycerides are low (below 70 mg/dL) or very high (above 400 mg/dL). It also obscures a critical distinction that has profound clinical implications: two patients can have the same LDL cholesterol concentration but vastly different numbers of LDL particles.
Patient A has an LDL of 110 mg/dL composed of large, buoyant LDL particles — fewer particles carrying more cholesterol each.
Patient B has an LDL of 110 mg/dL composed of small, dense LDL particles — more particles carrying less cholesterol each.
Both patients have identical LDL cholesterol. Patient B has dramatically higher cardiovascular risk. The standard lipid panel cannot distinguish between them. ApoB can.
What Is ApoB?
Apolipoprotein B is a structural protein that is present — exactly once — on the surface of every atherogenic lipoprotein particle:
Every LDL particle
Every VLDL particle
Every IDL particle
Every Lp(a) particle
Because each of these particles carries exactly one ApoB molecule, measuring serum ApoB gives you a direct count of the total number of atherogenic particles in your blood. This is particle number — which is what actually matters for atherosclerotic risk — not cholesterol concentration.
The mechanism is straightforward: lipoprotein particles cause atherosclerosis by crossing the endothelial lining of arteries and becoming retained in the arterial wall. The more particles in circulation, the more frequently this infiltration occurs. Particle number — measured by ApoB — is therefore the primary driver of atherosclerotic plaque formation.
The Evidence for ApoB Over LDL
The superiority of ApoB as a cardiovascular risk marker is not a fringe position. It is supported by decades of epidemiological research, multiple large prospective studies, and increasing consensus among preventive cardiologists and longevity physicians.
Key findings from the research literature include:
ApoB predicts cardiovascular events more accurately than LDL-C in multiple large cohort studies, including the INTERHEART study of over 27,000 participants across 52 countries — one of the largest cardiovascular risk factor analyses ever conducted.
Discordance between LDL and ApoB is common. Studies consistently show that 20–30% of patients have meaningfully discordant LDL and ApoB values — meaning their LDL underestimates or overestimates their actual particle burden. In patients with insulin resistance, metabolic syndrome, or low triglycerides, this discordance is particularly prevalent.
Patients with low LDL but high ApoB — the "discordant" group — have cardiovascular event rates that track with their ApoB, not their LDL. Their risk is higher than their LDL suggests. Without ApoB, this risk is invisible on a standard panel.
Statin therapy reduces both LDL and ApoB, but the residual ApoB level after treatment — not the residual LDL — is a better predictor of whether treatment is sufficient.
Who Has Discordant LDL and ApoB?
Discordance — where LDL underestimates particle burden — is particularly common in:
Patients with insulin resistance or metabolic syndrome. When insulin signaling is impaired, the liver produces more small, dense LDL particles. These particles carry less cholesterol per particle, so LDL cholesterol appears lower than the actual particle count would suggest. ApoB captures this accurately. LDL does not.
Patients with low triglycerides. Low triglycerides are often associated with small, cholesterol-poor LDL particles — meaning particle number is high relative to LDL cholesterol concentration. This is the pattern associated with a very low-carbohydrate diet, for example, where LDL can appear elevated but particle size is large and ApoB may be entirely normal.
Patients with high HDL. High HDL is generally protective, but it can mathematically inflate calculated LDL via the Friedewald equation in ways that don't reflect actual atherogenic particle burden.
Patients on testosterone replacement therapy. TRT modestly lowers HDL in some patients. This can alter calculated LDL in ways that don't accurately represent cardiovascular risk. ApoB provides a cleaner picture.
Post-menopausal women. The lipid profile changes significantly after menopause — including shifts toward smaller, denser LDL particles — making ApoB particularly valuable in this population.
How to Interpret Your ApoB Result
ApoB is measured in milligrams per deciliter (mg/dL).
Standard reference ranges:
CategoryApoB LevelOptimalBelow 80 mg/dLNear optimal80–99 mg/dLBorderline high100–129 mg/dLHigh130 mg/dL and above
Provena Care targets:
For patients with no established cardiovascular disease or diabetes, we target ApoB below 90 mg/dL as a general preventive goal. For patients with established cardiovascular disease, diabetes, or multiple risk factors, we target below 70 mg/dL — consistent with current ACC/AHA high-risk guidelines.
These targets reflect cardiovascular outcomes data, not population averages. The reference range on your lab report represents the distribution of ApoB in the general population — not the levels associated with lowest cardiovascular risk.
ApoB and Lipoprotein(a) — The Other Missing Marker
Lipoprotein(a), or Lp(a), is a genetically determined lipoprotein that carries additional atherogenic and thrombotic risk beyond what ApoB captures. Lp(a) levels are largely set by genetics — diet and lifestyle have minimal effect — and elevated Lp(a) is present in approximately 20% of the population.
Lp(a) is counted within ApoB (each Lp(a) particle carries one ApoB molecule), but because it carries additional risk through a separate mechanism, it should be measured separately at least once in every adult.
Most patients have never had Lp(a) measured. At Provena, we include Lp(a) in our baseline cardiovascular assessment for Performance and Elite members as part of the comprehensive metabolic panel.
ApoB at Provena Care — What We Order and When
For Core members, we include ApoB in our recommended annual add-on panel discussion and can order it alongside your standard labs at member-preferred pricing.
For Performance members, ApoB is included in the Core Performance Lab Panel as a standard marker, along with Lipoprotein(a) as a baseline measurement.
For Elite members, ApoB and Lp(a) are included in both comprehensive optimization panels per year, along with advanced lipid particle testing.
For all patients, ApoB results are reviewed directly with your provider — not sent to a patient portal with a checkmark that says "normal."
What to Do If Your ApoB Is Elevated
The management of elevated ApoB depends on the underlying cause — which is why the clinical context of the result matters as much as the number itself.
If elevated ApoB is driven by insulin resistance and high particle number: The primary intervention is metabolic — reducing refined carbohydrates, improving insulin sensitivity through diet and exercise, and addressing underlying inflammatory drivers. This often reduces ApoB substantially without medication.
If elevated ApoB persists despite lifestyle optimization: Statin therapy, ezetimibe, and newer agents including PCSK9 inhibitors are highly effective at reducing ApoB. The choice of agent and target ApoB level is individualized based on overall cardiovascular risk.
If discordance exists between low LDL and high ApoB: This is a situation where treating LDL alone would leave cardiovascular risk unaddressed. ApoB-directed treatment is essential.
If Lp(a) is significantly elevated (above 75–100 nmol/L): This warrants more aggressive management of all other modifiable cardiovascular risk factors — blood pressure, LDL, ApoB, inflammation, metabolic health — since Lp(a) itself currently has limited direct treatment options outside of clinical trials.
The Bottom Line
Your standard lipid panel is a starting point, not a complete cardiovascular risk assessment. LDL cholesterol is a useful marker that has saved lives through decades of statin prescribing. It is also an imprecise tool that misses meaningful cardiovascular risk in a substantial minority of patients.
ApoB is not a new or experimental marker. It is a direct measurement of atherogenic particle burden, supported by more than 40 years of research and increasingly recommended by cardiovascular societies worldwide. It is, in most patients, a more accurate reflection of cardiovascular risk than the LDL number your standard panel reports.
At Provena Care, we order it because our patients deserve a complete picture of their cardiovascular health — not just the numbers that fit on a standard requisition form.
Provena Care 10251 SW 72nd St, Suite 106 · Miami, FL 33173 305.395.7108 · info@provenacare.com
ApoB and Lp(a) are included in Performance and Elite membership lab panels. Core members can add these markers at member-preferred pricing. View membership plans.