The Complete Guide to Peptide Therapy: What Researchers and Clinicians Are Discussing in 2026
Inside look at Peptide Therapies, from ProveCare Clinicaal team. ssssssGLP-1s, BPC-157, TB-500, GHK-Cu, sermorelin, tesamorelin, NAD+, stacks, with strong "not medical advice" disclaimers
PATER ATTIA, MDNAD+TESTOSTERONEDEEP SLEEPCMPHEART HEALTHPEPTIDE THERAPYLONGEVITYSEMAGLUTIDEPEPTIDESANTI-AGINGSLEEP OPTIMIZATIONLONGEVITY MEDICINEGLP-1BCP-157TB-500SERMORELINTESAMORELINGHK-CU
Provena Care Clinical Team
6/14/202613 min read
The Complete Guide to Peptide Therapy: What Researchers and Clinicians Are Discussing in 2026
Peptide therapy has moved from a niche topic discussed mostly in bodybuilding and anti-aging forums to a mainstream conversation featured on some of the largest health and science podcasts in the world. Andrew Huberman's October 2024 episode with Dr. Craig Koniver — a physician who has worked extensively with peptide and hormone protocols — brought terms like "ipamorelin," "BPC-157," and "tesamorelin" into living rooms across the country. Dr. Peter Attia has discussed GLP-1 medications extensively across multiple episodes, examining their mechanisms, benefits, and risks in detail. And peptides more broadly have become a recurring topic across the longevity media landscape.
This guide is intended as a comprehensive, educational overview of the peptides most frequently discussed by researchers, physicians, and podcasters in this space — what they are, what people report using them for, and what the current research landscape looks like. This is one of the most important things to understand up front: this article describes what is being discussed publicly. It does not constitute medical advice, and it is not an endorsement or recommendation for any specific peptide. Full disclaimers are provided at the end of this article, and we encourage you to read them carefully.
With that framing in place, let's dig in.
What Are Peptides, Exactly?
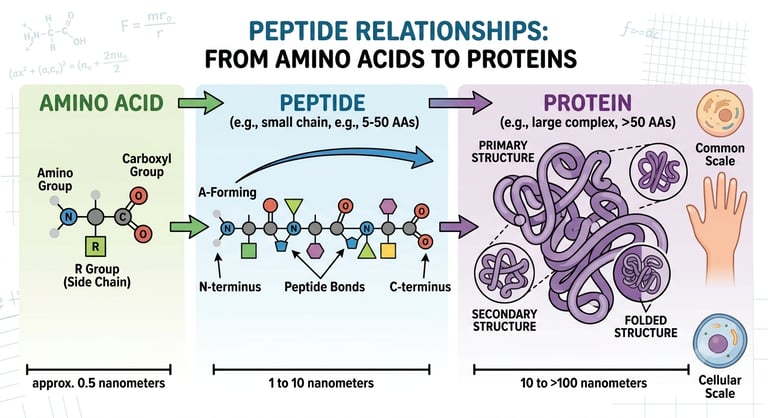
Peptides are short chains of amino acids — the same building blocks that make up proteins, just in smaller chains (generally fewer than 50 amino acids, compared to proteins which can be hundreds or thousands). Many peptides occur naturally in the body and play roles as hormones, signaling molecules, or components of the immune system. Insulin, for example, is a peptide hormone.
What's changed in recent years is the ability to manufacture specific peptides that mimic or influence these natural signaling pathways — which is why so many of the peptides discussed in longevity circles are related to growth hormone signaling, tissue repair, metabolic regulation, and inflammation.
GLP-1 Receptor Agonists: The Most-Studied Category
No discussion of peptides in 2026 would be complete without addressing GLP-1 receptor agonists — medications like semaglutide and tirzepatide, which have become some of the most talked-about medications in modern medicine.
What Dr. Peter Attia Has Said
Dr. Peter Attia has discussed GLP-1 medications across several episodes, including dedicated AMA (Ask Me Anything) episodes focused specifically on this drug class. His commentary has covered several recurring themes:
• Mechanism — GLP-1 receptor agonists mimic a naturally occurring gut hormone (glucagon-like peptide-1) that affects appetite regulation, gastric emptying, and insulin secretion. This is why they were originally developed for type 2 diabetes before their effects on weight became a major focus.
• Efficacy — Clinical trials have shown substantial average weight loss in many participants, which is part of why these medications have generated so much attention.
• The muscle loss concern — One of Dr. Attia's most consistently repeated points is that a meaningful portion of weight lost on GLP-1 medications can come from lean mass (muscle), not just fat — which is a significant concern from a longevity perspective, since muscle mass is strongly associated with healthy aging, metabolic health, and functional independence later in life. This is why Attia has emphasized that adequate protein intake and resistance training are not optional extras during GLP-1 use — they're essential to protect muscle mass during weight loss.
• Post-discontinuation effects — Dr. Attia has also discussed what happens after people stop taking GLP-1 medications, noting that appetite and weight can rebound for many people, which raises questions about whether these medications are best thought of as a short-term tool or a longer-term (potentially indefinite) intervention for some individuals — a question that's still being actively studied and debated.
• Side effects — Commonly discussed side effects include nausea, gastrointestinal symptoms, and in rarer cases, more serious concerns that should be discussed with a prescribing physician.
What People Report Using GLP-1s For
Based on public discussion, people pursuing GLP-1 therapy commonly describe goals related to:
• Weight management, particularly for those who have struggled with traditional approaches
• Appetite regulation and reduced food preoccupation
• Improvements in markers related to metabolic health (blood sugar, in particular)
Again — these are commonly reported goals discussed publicly, not claims that any specific outcome will occur for any specific person. GLP-1 medications are prescription medications that require medical supervision, and decisions about their use should be made with a physician who can evaluate your full health picture.
BPC-157: The "Body Protection Compound"
BPC-157 is a peptide that has generated significant interest in discussions about tissue repair and recovery. Peter Attia discussed BPC-157 in an episode featuring Derek (from the channel More Plates More Dates), and the framing in that conversation is instructive: Attia approached the topic with caution, describing the broader peptide space as something of a "Wild West" — meaning there's significant public interest and anecdotal enthusiasm, but the regulatory and research landscape lags behind.
What People Discuss Regarding BPC-157
In public discussion, BPC-157 is most often associated with conversations about:
• Soft tissue recovery — tendons, ligaments, and muscle
• Gut health discussions, given that BPC-157 was originally derived from research into a protective compound found in gastric juice
• General recovery support after injury, in anecdotal and forum-based discussion
The Regulatory Reality
It's important to be direct about something here: BPC-157 is not an FDA-approved drug. In recent years, the FDA has taken regulatory action restricting compounding pharmacies from producing BPC-157 for human use, specifically citing safety concerns related to the lack of adequate human research. This is a meaningfully different regulatory status than, for example, sermorelin or tesamorelin (discussed below), which have or have had FDA-approved indications. Anyone considering BPC-157 should be aware of this regulatory landscape and discuss it openly with a knowledgeable physician.
TB-500: Often Discussed Alongside BPC-157
TB-500 is a synthetic version of a naturally occurring peptide fragment derived from a protein called thymosin beta-4. In public discussion, it's frequently mentioned in the same breath as BPC-157, often as part of a "recovery stack," with people describing interest in its potential role in tissue repair and recovery from injury.
Like BPC-157, TB-500 exists in a research landscape with limited large-scale human clinical trials, and it carries similar regulatory considerations. The pattern across this category of peptides — TB-500, BPC-157, and others sometimes grouped under "research peptides" — is consistent: significant anecdotal and online interest, mechanistic plausibility based on how these molecules behave in lab and animal research, but a meaningfully smaller human evidence base compared to more established therapies.
GHK-Cu: The Copper Peptide
GHK-Cu (glycyl-histidyl-lysine bound to copper) is a naturally occurring copper-binding peptide that has been studied primarily in the context of skin health and wound healing — it's a common ingredient in some cosmetic and dermatological formulations, where its potential role in collagen production and skin repair has been a topic of interest for years, predating the current wave of peptide interest.
In the broader longevity and peptide conversation, GHK-Cu is sometimes discussed in relation to:
• Skin appearance and texture, in topical formulations
• General discussions about tissue repair, drawing on its longer history in dermatological research
GHK-Cu has a somewhat different profile than peptides like BPC-157 or TB-500 in that it has a longer track record in topical/cosmetic applications, though systemic (injectable) use is part of the broader "research peptide" conversation with the same caveats about limited large-scale human trials for that use case.
Sermorelin and Tesamorelin: Growth Hormone Secretagogues
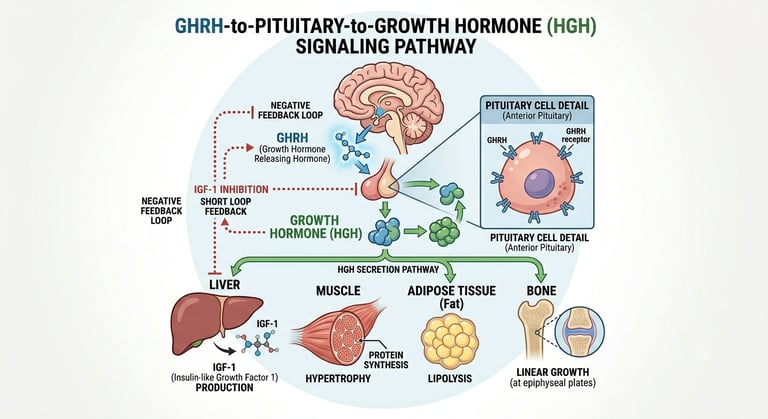
This category of peptides works differently than the ones discussed above. Rather than acting directly on tissue repair pathways, sermorelin and tesamorelin are growth hormone-releasing hormone (GHRH) analogs — meaning they signal the pituitary gland to produce and release more of the body's own growth hormone, rather than introducing growth hormone directly.
Sermorelin
Sermorelin has an FDA-approved history — it was originally approved for diagnosing and treating growth hormone deficiency, including in children with short stature. In adult off-label discussion, sermorelin has been associated with conversations about:
• Sleep quality — because growth hormone release naturally peaks during deep sleep, and GHRH analogs are often discussed in relation to supporting this natural rhythm
• Body composition discussions — muscle and fat ratio conversations in the context of overall metabolic health
• General discussions about supporting the body's natural growth hormone production rather than replacing it
Dosing protocols discussed in public conversation (including Dr. Koniver's discussion with Huberman) have referenced approaches like 200-400 mcg taken at night, several times per week rather than every single night — with the rationale being to avoid desensitizing the pituitary's response over time (a concept sometimes referred to as receptor downregulation).
Tesamorelin
Tesamorelin is also a GHRH analog, but it has a notable distinguishing feature discussed by Dr. Koniver: it appears to have a more specific effect on visceral fat — the fat stored around abdominal organs, which is more strongly linked to metabolic health concerns than subcutaneous fat. Tesamorelin has an FDA-approved indication for reducing excess abdominal fat in a specific clinical population (people with HIV-associated lipodystrophy), which gives it a somewhat more established regulatory and research footing than peptides like BPC-157 or TB-500, even though its broader off-label use for general visceral fat reduction is a separate conversation from its approved indication.
NAD+ and Peptide Conversations
NAD+ (nicotinamide adenine dinucleotide) isn't technically a peptide, but it frequently comes up in the same conversations because it's part of the broader cellular health and longevity toolkit discussed by researchers like Dr. David Sinclair. As covered in our dedicated article on NAD+ IV therapy, NAD+ is central to mitochondrial energy production and the activity of sirtuins — proteins involved in DNA repair and cellular stress responses.
In stack discussions, NAD+ support (whether via IV therapy or oral precursors like NMN/NR) is sometimes paired with peptide protocols as part of a broader "cellular health" framing — the idea being that supporting mitochondrial function and tissue repair pathways simultaneously may be complementary, though this combined approach has even less dedicated research than the individual components.
Peptide "Stacks": What Dr. Koniver Discussed With Huberman
One of the most-referenced parts of the Huberman/Koniver conversation was the discussion of specific peptide combinations, or "stacks." It's worth walking through these as they were discussed publicly — again, purely as a description of what's being talked about, not a recommendation.
The "Bedtime Stack"
This combination, as discussed, generally involves:
• Ipamorelin (around 100 mcg) — a growth hormone secretagogue similar in category to sermorelin
• Sermorelin or tesamorelin — with the choice between them often framed around whether visceral fat is a specific area of focus (tesamorelin) versus a more general approach (sermorelin)
• Pentadeca arginate (PDA) (around 500 mcg) — a peptide discussed in the context of anti-inflammatory effects and potentially upregulating growth hormone receptor sensitivity
The rationale discussed for combining these at bedtime ties back to the natural nighttime pattern of growth hormone release during deep sleep — the idea being to work with, rather than against, the body's existing rhythms.
The "Fat Loss Variation"
A variation on this discussed in the same conversation swaps in:
• Tesamorelin (for its visceral fat-specific signaling)
• Ipamorelin
• BPC-157 or PDA — discussed in the context of supporting recovery, particularly if the person is also engaged in resistance training or has joint-related concerns
How to Think About Stacks
The honest framing here is important: combining multiple peptides multiplies the number of unknowns, not just in terms of individual peptide research (which, as discussed above, varies widely in quality and quantity), but also in terms of how these compounds may interact with each other, with other medications, and with an individual's specific health history. Stacks discussed publicly represent what individuals and some physicians have reported trying — they are not standardized, FDA-evaluated protocols.
A Word on "What People Say They Use Peptides For"
Throughout this article, we've tried to be careful about language — describing what's discussed, reported, or studied, rather than making claims about what peptides "do" for any individual. This distinction matters for a few reasons:
1. Individual variation is enormous. Two people using the same peptide at the same dose can have very different experiences, and anecdotal reports — even widespread ones — aren't the same as controlled evidence.
2. The regulatory landscape varies dramatically by peptide. As discussed above, sermorelin and tesamorelin have FDA-approved histories (even if current off-label use differs from those approved indications), while BPC-157 and TB-500 currently face FDA restrictions on compounding for human use. Lumping all "peptides" together obscures these important differences.
3. Quality and sourcing matter enormously, and this is an area where the "Wild West" framing Attia used is particularly apt — peptides obtained outside of a regulated medical supply chain carry risks related to purity, dosing accuracy, and sterility that are separate from the question of whether the peptide itself has merit.
How Provena Care Approaches Peptide Therapy
Given everything discussed above, here's how we think about peptide therapy as part of our longevity membership:
• We focus on peptides with the strongest regulatory and research foundation for the specific goals a patient is interested in, and we're transparent about where the evidence is more or less established for any given compound.
• Sourcing matters. Peptides used in our protocols come through licensed pharmacy channels (503 A/B) with appropriate quality and sterility standards — not unregulated "research chemical" suppliers.
• Everything is individualized and monitored. Peptide therapy, where appropriate, is paired with relevant lab work and follow-up, not a one-size-fits-all prescription.
• We'll tell you when something isn't appropriate. If a patient asks about a specific peptide that we believe carries more risk than evidence supports for their situation, our clinical team will have that direct conversation — our goal is your long-term health, not just satisfying a request.
If you're curious about whether peptide therapy might be relevant to your goals — whether that's related to recovery, body composition, sleep, or general longevity support — the right first step is a conversation with our clinical team, where we can discuss your health history and what realistically makes sense for you.
Why This Topic Has Become Mainstream
Five years ago, peptide therapy was largely confined to longevity-focused medical practices, anti-aging clinics, and corners of the bodybuilding community. Today, it's a recurring topic on some of the most-listened-to podcasts in the world — a shift that reflects both growing public interest in proactive health management and the broader cultural momentum behind the longevity movement that figures like Attia, Huberman, and Sinclair have helped build.
Joe Rogan's podcast has played a role in this shift as well, with peptide-related topics surfacing in conversations with guests across fitness, medicine, and longevity research. The throughline across these various podcast conversations isn't a single unified recommendation — it's closer to a shared curiosity about an emerging category of compounds, paired with a recurring acknowledgment that the science is still catching up to the public interest. That gap between interest and evidence is exactly why a guide like this one exists: to help separate what's being talked about from what's been established.
The Role of Lab Work and Monitoring
One theme that doesn't always come through in podcast-length conversations, but that's central to how peptide therapy is approached in a clinical setting, is the role of baseline testing and ongoing monitoring. For growth hormone secretagogues like sermorelin and tesamorelin, this can include monitoring IGF-1 levels (a downstream marker of growth hormone activity), since the goal of these therapies is generally to support levels within a healthy physiological range — not to push them beyond it.
For GLP-1 medications, monitoring typically includes metabolic markers (blood glucose, HbA1c) as well as tracking body composition changes over time — which is part of why Attia's point about resistance training and protein intake matters so much. A number on a scale doesn't tell you whether the weight being lost is fat or muscle, but body composition testing (such as DEXA scans) can.
For peptides discussed in the recovery and tissue-repair category, monitoring is often more individualized — tracking symptoms, function, and recovery timelines relative to a person's specific situation, since there typically aren't standardized lab markers in the way there are for hormone-related peptides.
The broader point: peptide therapy, when approached clinically, isn't a "set it and forget it" intervention. It involves a starting point, a plan, and check-ins along the way — which is a meaningfully different experience than self-directed use based on what's been discussed online.
Cost, Access, and the Membership Model
One question that comes up frequently is how peptide therapy fits into the cost structure of a longevity-focused practice. Unlike many services covered by traditional insurance, peptide therapy — along with NAD+ IV therapy and many hormone optimization services — typically falls outside standard insurance coverage, which is part of why these services are often offered through membership-based models like the one Provena Care offers.
This isn't unique to peptides; it reflects a broader pattern in how proactive, longevity-focused care is currently structured in the U.S. healthcare system, where insurance is generally built around treating diagnosed disease rather than optimizing function in the absence of disease. Understanding this distinction can help set realistic expectations about cost and access when exploring these options.
Frequently Asked Questions
Are peptides legal?
The legal and regulatory status varies significantly by specific peptide. Some (like sermorelin and tesamorelin) have FDA-approved histories for certain indications. Others (like BPC-157) have recently faced FDA restrictions on compounding for human use. This is a rapidly evolving regulatory area, and "peptides" as a category shouldn't be thought of as a single legal status.
Do I need a prescription for peptide therapy?
Peptides used in a clinical setting, like the ones discussed in our longevity membership, are provided through appropriate medical channels with physician oversight — this is different from peptides purchased online from unregulated sources, which carry additional risks.
How long do peptide protocols typically last?
This varies enormously depending on the specific peptide, the goal, and individual response, and is something to discuss directly with your provider rather than something with a universal answer.
Is GHK-Cu the same as the other "research peptides" discussed in this article?
Not exactly — GHK-Cu has a longer history in topical/cosmetic dermatological applications compared to peptides like BPC-157 and TB-500, though systemic use falls into the same broader "research peptide" category with similar evidence limitations.
Important Disclaimers
This article is for educational and informational purposes only and does not constitute medical advice, diagnosis, or treatment. The information presented reflects publicly available research, regulatory information, and commentary from independent researchers, physicians, and podcast hosts. It is intended to describe topics of public discussion, not to recommend, endorse, or provide instructions for the use of any specific peptide or compound.
This article does not make claims that any peptide discussed will produce any specific outcome for any individual. References to what "people report" or "discuss" reflect publicly available anecdotal and research discussion, not verified clinical outcomes, and should not be interpreted as evidence of efficacy or safety for any individual's specific situation.
Regulatory status varies by peptide and may change. Some peptides discussed in this article (such as BPC-157) are subject to FDA restrictions regarding compounding for human use. Others (such as sermorelin and tesamorelin) have specific FDA-approved indications that differ from broader off-label discussion. Readers should not assume any peptide discussed is legal, available, or appropriate for their use based on this article.
Peptide therapy carries risks, including but not limited to injection site reactions, hormonal effects, interactions with other medications or health conditions, and risks associated with product quality and sourcing — particularly for peptides obtained outside regulated medical supply chains.
GLP-1 medications are prescription medications that require evaluation and ongoing supervision by a licensed physician. They are not appropriate for everyone and carry their own risk profile, including gastrointestinal side effects and considerations around lean mass preservation during weight loss.
Nothing in this article should be used as a substitute for individualized medical advice from a qualified healthcare provider. Before considering any peptide therapy, GLP-1 medication, or related intervention, consult a licensed physician who can evaluate your complete health history, current medications, and individual risk factors. If you are pregnant, breastfeeding, have a history of cancer, have a chronic medical condition, or are taking other medications, this conversation is especially important.
Provena Care's peptide-related services are provided only through appropriate medical evaluation and oversight by our clinical team, and we do not provide peptides or related guidance outside of that clinical relationship.